Our easy-to-read fact sheets provide clinicians with reliable information to share with patients and their caregivers.
Biomedical therapy for autism spectrum disorder (ASD) is becoming increasingly popular as a complementary treatment option to traditional medication regimes, yet many patients are still unclear about what biomedical therapy entails. Therefore, the following fact sheet provides a helpful overview of biomedical therapy for ASD and answers commonly asked questions.
Autism Spectrum Disorder
Autism spectrum disorder (ASD) is a neurodevelopmental disorder associated with impairment in social communication and interactions as well as the presence of restricted, repetitive behaviors.1 It is influenced by both genetic and environmental factors, though the direct cause is still unknown.2
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) is considered the gold standard for ASD diagnosis. The diagnostic criteria for ASD are graded on a severity scale by the level of support needed, in which Level 1 requires support, Level 2 requires substantial support, and Level 3 requires very substantial support.2
Common Treatment Options for Autism
Because ASD occurs on a spectrum, treatment options can vary with each patient depending on their unique set of symptoms. There is no curative treatment for ASD, but the management of ASD takes on a multifaceted approach that includes occupational, behavioral, speech, and play therapies. Psychosocial interventions can also help improve specific behaviors, such as language and social engagement.3
Although there are no medications directly indicated for the treatment of ASD specifically, many individuals receive medication for comorbidities associated with their diagnosis. Patients with ASD may take medication for irritability, aggression, hyperactivity, and seizures that may co-present with the condition.2 Some examples of the common medications used to manage these other symptoms and disorders may include:4
Biomedical therapy is a specific treatment approach that considers the underlying biological basis of a condition and targets physiological impairment.5 The goal of biomedical therapy for autism is to optimize physiological factors impacting brain function and development to treat symptoms and improve patient functioning.
Research indicates that ASD is associated with deficits in mitochondrial metabolism and oxidative stress as well as abnormalities in the regulation of the following essential metabolites:6
Folate
Tetrahydrobiopterin
Glutathione
Cholesterol
Carnitine
Branch chain amino acids
Biomedical therapy can be categorized based on the pathophysiological process they target.
Mitochondrial Dysfunction
The mitochondria generate energy for cellular processes. When the mitochondria is impaired, it can lead to developmental delays, muscle weakness, and neurological problems.6 Individuals with ASD who have mitochondrial dysfunction often have more severe behavioral and cognitive deficits, relative to those with typical mitochondrial function. Treatments may include:6
Antioxidants, such as vitamin C and N-acetyl-L-cysteine
L-carnitine
Multivitamins containing vitamin B, vitamin E, co-enzyme Q10
Folate Metabolism
Folate is naturally found in the human body and helps to regulate the absorption of vitamin B. However, individuals with ASD may have genetic modifications in the folate pathway which leads to a decrease in available folate in the brain, known as cerebral folate deficiency. Lack of folate causes symptoms such as fatigue and muscle weakness. Patients with folate irregularity are treated with folinic acid for neurological, behavioral, and cognitive improvements.6
Redox Metabolism
Redox reactions are necessary for many biological functions. Evidence has shown that individuals with ASD may have abnormal redox metabolism which could lead to oxidative damage in areas of the brain responsible for speech, emotion, and social behavior. Several treatments for oxidative stress are available, including:6
Vitamin or mineral supplements containing antioxidants, co-enzyme Q10, and vitamin B
Subcutaneous injections of methylcobalamin (a form of vitamin B12)
Oral folinic acid
Tetrahydrobiopterin supplementation
N-acetyl-L-cysteine
These treatment options can help improve many common ASD symptoms, including hyperactivity, tantrums, sensory-motor skills, irritability, and even sleep and gastrointestinal symptoms.
Tetrahydrobiopterin Metabolism
Tetrahydrobiopterin (BH4) is naturally found in the body and is necessary for multiple important metabolic pathways. Abnormalities in BH4 are prominent in ASD, as the disorder is associated with a lack of oxidative stress needed for BH4 pathways. Treatment for BH4 metabolic dysfunction is primarily the use of sapropterin, a synthetic form of BH4. Sapropretin has been shown to improve cognitive ability, communication, adaptability, verbal expression, and social function in patients with ASD.6
Frequently Asked Patient Questions
At what stage should I consider biomedical therapy for autism?
Because ASD is a lifelong condition that occurs on a spectrum, there is no standard timeline for when a treatment should be started.7 Interventions are tailored to the patient’s specific needs. Although supplements are generally safe and well tolerated, they can have interactions with certain medications. Speak with your healthcare provider when making decisions on treatment options as it is important to keep track of your medications to monitor improvement and prevent adverse medication interactions.
How long does it take to see improvement?
When evaluating treatment success, it is important to consider what symptoms or conditions are being targeted. For example, some patients may be seeking treatment to sleep better or decrease their repetitive behaviors. Tracking progress by logging symptoms and improvements can help you and your provider gain an accurate measure of your treatment response. Improvements may not be seen immediately, especially as certain medications can take time to show measurable effects. Your symptoms may fluctuate over time, so consistent medication adherence is necessary to improve your chances of overall improvement.8
Are there side effects associated with these treatments?
All of the biomedical treatments mentioned throughout this fact sheet are generally considered safe and well-tolerated. However, there are minor side effects for some of these treatments, as detailed below:
Patients taking L-carnitine have expressed slight gastrointestinal issues. Symptoms such as nausea, vomiting, and abdominal cramps are usually experienced when the supplement is taken at night on an empty stomach. To minimize these symptoms, these supplements can be taken after a meal and your time of dosing can be adjusted.6
Some patients taking high-dose folinic acid may experience increased irritability, insomnia, or gastroesophageal reflux when co-administered with other medications, such as antipsychotics.6
Individuals taking N-acetyl-L-cysteine may experience mild side effects such as constipation, fatigue, daytime drowsiness, or increased appetite.6
Not all patients respond to treatment options in the same way. Patients should speak with their providers to discuss their treatment plan and any potential side effects they may experience.
Thru-hiking is a long-term endeavor in which a hiker walks a long-distance trail with continuous footsteps from one end to another.1 There is limited data to provide evidence-based recommendations for assessing patient readiness for long-term hiking. Anecdotes from thru-hikers suggest that many health care providers respond with “Wow, great!” but do not provide in-depth evaluation or counseling. The lack of understanding of the hardships hikers encounter during and after-thru hike can leave hikers without adequate preparation medical treatment.
Halfwayanywhere.com is a site that collects voluntary data from thru-hikers on the Pacific Crest Trail (PCT), one of the most popular thru-hikes in the US that runs 2650 miles. Due to the voluntary nature of the survey, the data on the site is not expected to be 100% accurate; however, it provides a useful overview of thru-hikers. Of 2022 hikers, 55.3% were male, with females and genderqueer, transgender females, and agender hikers representing the rest. Hikers of all ages hike the PCT; 37.17% were under 30 years; 21.58% were over 50 years; and 41.24% were between 30 and 50 years. Regarding their educational background, 80.4% had some post-secondary education, with 47.5% having a bachelor’s degree. For 43.1% of these hikers, this was their first thru-hike. On a scale of 1 to 10, with 10 being the most fit, the respondents rated their average fitness level at 5.8 prior to the hike.2
"
… a thorough mental status and goal assessment should be included as the re-adjustment to non-hiking life can be difficult for some.
The failure rate for thru-hikers of the PCT is about 50%.3 Some reasons for this high rate of non-completion include injury, weather (such as fires or snow), work, family, feeling defeated, and illness.4 Many people take on the endeavor of a thru-hike with a romantic notion of campfires and sleeping under the stars without seriously considering the hardships undergone throughout the journey (heat, cold, many miles, carrying a heavy pack, and wear and tear on the body). Sometimes the reality of the hike clashes with the pre-conceived notions of the hike, leading to depression and frustration on the trail. In addition, there has been documentation of post-trail depression5. The causes are unknown, but are thought to be related to lack of endorphins, lack of goals, returning to the reality of day-to-day life and responsibilities, and other cultural responsibilities once off trail.
Questions for Providers to Consider
These concerns raise the need for health care providers to assess and counsel patients presenting for a physical prior to a thru-hike. A full assessment is important, with careful consideration given to cardiovascular, respiratory, musculoskeletal, and neurologic examinations. This assessment should be focused on areas that may hinder the progress of the hiker, including medical diagnoses. In addition, a thorough mental status and goal assessment should be included as the re-adjustment to non-hiking life can be difficult for some.
Patient with diabetes, for example, will need to know how to adjust their insulin; that their glucose meter must be kept in their sleeping bag together with electronics and water filters to keep from freezing; what glucose limits are right for them; and how much glucose to take if they have a crash. Remind your patients with diabetes that having higher glucose levels is always better than hypoglycemia. This discussion may also result in modification of the amount of daily long-acting insulin used.
Female hikers have particular health concerns that we have addressed in an earlier article.
Diet
Proper nutrition is key in order for the hiker to complete their event.6 Regardless of the hiker’s dietary style, the primary nutritional considerations are total calories and quality of calories. Thru-hikers may spend several hours on the trail each day, potentially raising an individual’s energy expenditure 2- to 3-fold. This may be compounded by the weight of the hiker’s pack (average 20% of bodyweight), increasing the energy expenditure and workload further.7 One key to a successful hike is consuming enough calories to match the increased demands.
Consistently consuming fewer calories relative to the increased demands may lead to low energy availability (LEA), which can lead to serious consequences. For female hikers, this can mean menstrual dysfunction and reduction in bone mineral density; for male athletes, a reduction in ferritin and vitamin D concentrations.8 Appropriate total calories are essential for thru-hikers as intake directly impacts energy availability, recovery processes, and total body-mass fluctuations throughout the journey. The use of technology on the trail to help monitor calorie expenditure and consumption is available; however, these tools can sometimes incorrectly estimate caloric needs. Finally, consider referring the hiker to a nutrition professional who specializes in sports, ultra-endurance exercise, or similar fields to help the hiker prepare appropriately.
Weight loss will likely occur, but the hiker should be alerted to signs and symptoms of when this weight loss may interfere with health, performance, and recovery. Each hiker has a different body composition, so the actual amount of weight loss will be variable. Attention should be paid to decreasing performance, loss of energy, or change in mood as these could be indicators of excessive weight or muscle loss. Identifying weight loss may be a challenge since scales are not always available. Other objective and subjective weight management tools, such as the fit of clothing and visual inspection in mirrors, can be used to help the hiker track weight fluctuations.
Hikers should be encouraged to explore calorically dense food options that emphasize essential nutrients such as oils, nuts, seeds, dairy, etc; and complete protein food sources such as tuna, salmon or chicken packets, beef jerky, dairy, and protein bars. Once total calories are considered, portions and meal timing can be individualized. Meals are recommended on a more frequent schedule. All meals and snacks should emphasize total calories and nutrient density. Particular attention should be paid to total dietary fat and dietary protein as these are required for recovery and structural integrity. When considering protein, find ways to encourage the hiker to consume complete proteins (animal protein sources) or complementary protein sources (a mix of plant proteins plus a branched-chain amino acid supplement) to help support recovery needs, reduce exercise-induced inflammation, and manage oxidative stress.
Hydration
Proper hydration is paramount to performance and recovery. Currently, hydration guidelines are personalized using the weight, urine, thirst (WUT) model by Sekiguchi et al.9 The WUT model takes into consideration total body weight, urine color, and an individual’s thirst level as indicators for hydration.
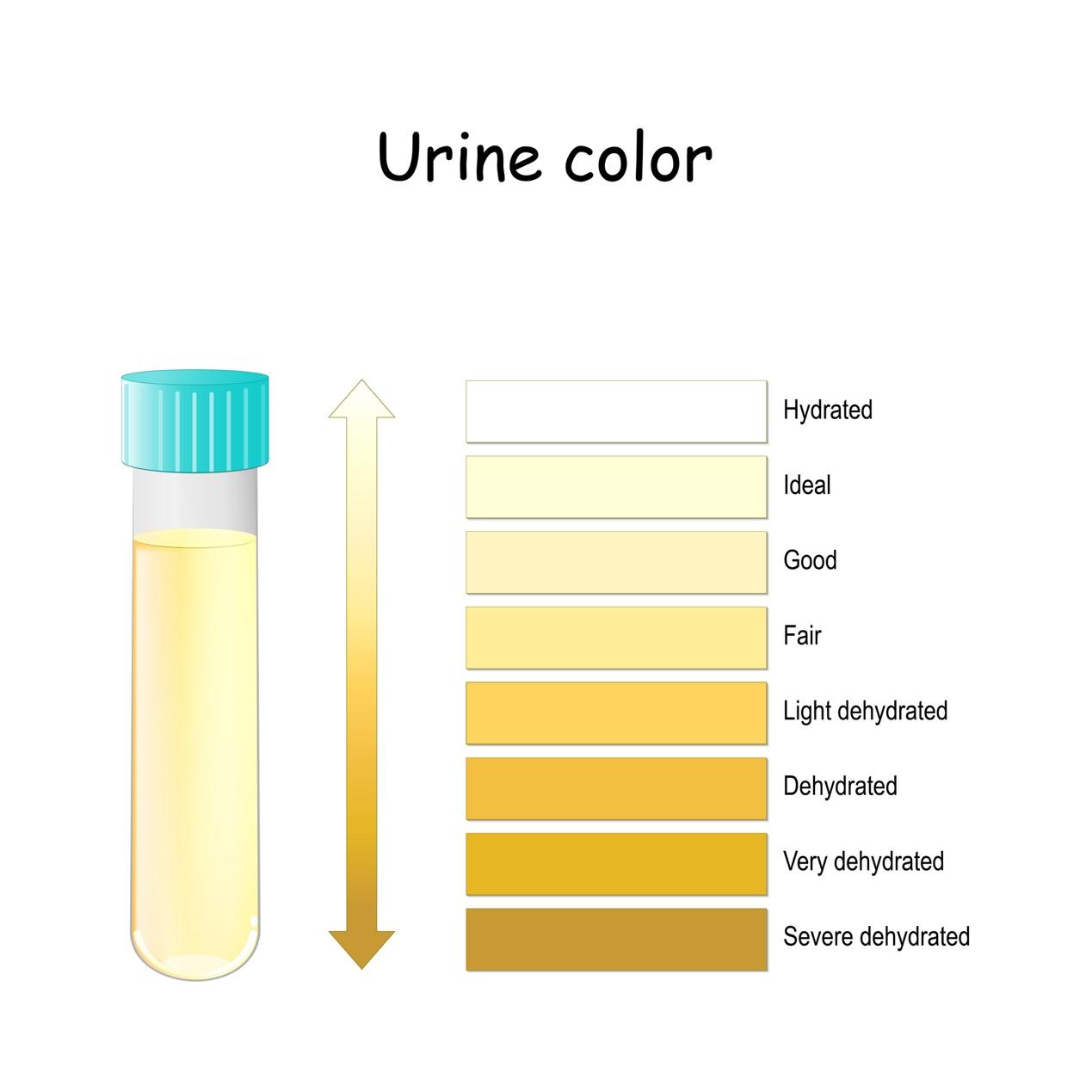
While exact intake needs are individualized, a starting point could be 1 liter for every 5 miles hiked. The hiker should be instructed to personalize from there. Another method of assessing hydration on the go is the use of the urine color chart (Figure 1).10
Temperature and elevation also have an impact on the need for hydration and should be included in the planning. Alert your patients to the need to monitor their urine for odor, color, and amount. Urine should not have any odor. An odor in urine could be a sign of urinary tract infection (UTI). The goal is for urine to be light yellow with a good flow. Any deviation from this may indicate poor hydration and should be addressed with increased fluids and possibly electrolytes.
Electrolyte imbalances are a concern due to the extended daily exercise, environmental conditions, and decreased intake of foods with high water content. While electrolytes are encouraged, personal consultation should be provided for each individual to ensure electrolyte intake does not interfere with any health or medical conditions.
There are a variety of sources on the market that can aid in electrolyte replenishment. Sodium is the primary electrolyte lost in sweat, so ensuring thru-hikers replenish sodium each day is vital. Magnesium is directly involved in skeletal muscle recovery so hikers may consider increasing magnesium intake. Some products are readily available to assist with electrolyte supplementation. Electrolyte supplementation should provide sodium, potassium, chloride, and magnesium. Examples of these products are Nuun Sport Tablets, Drip Drops, Liquid IV, and some MIO products.
Medications and Devices
As health care providers we can provide hikers with a list of medications that will be helpful in dealing with some of the frequent issues they might encounter on the trail. Careful instructions and explanations on how to take these medications are needed. If a hiker uses hearing aids or glasses, they should plan for what to do if they are lost or broken.
Ibuprofen is perhaps the best medication for aches and pains. Contraindications for these should be explored with the patient and considerations on taking the medication should be discussed.
Antidiarrhea medications are helpful (ie, loperamide). Discussion about when and how to take them is recommended, including when to start and for how long. Two common causes of diarrhea on the trail, Giardia and Salmonella, can be disastrous without treatment. Hydration is also a concern if the hiker develops diarrhea. Regular use of stool softeners may help to maintain the stool consistency. Bismuth tablets are easy to carry and may be helpful with gastrointestinal complaints.
Allergic reactions to seasonal allergens, or to bug bites, including mosquitoes, bees, ants, or spiders, benefit from small dosages of oral and/or topical diphenhydramine. Alert the hiker to potential side effects.
In case of exposure to poison ivy, poison oak, or sumac, alert patients that it could take hours or even days for the rash to appear. Zanfel is a topical cream known to minimize the symptoms associated with exposure to these plants. Some patients might require steroids, depending on the severity of the reaction.
Prescriptions as Prophylactic Medications
The antibiotic cephalexin can be used for UTIs, sinus infections, skin infections, and diarrhea. Ciprofloxacin can also be prescribed for these conditions; however, the risk of photosensitivity and tendon rupture/tendonitis makes this the second choice. Azithromycin is another drug used for traveler’s diarrhea and can be prescribed with instructions on how and when to take. Bactrim DS can also be prescribed for the development of traveler’s diarrhea, UTI, sinus infection, or skin infections.
Knowing which infections are endemic to the area is important. Trails like the Appalachian Trail are known for tickborne diseases such as Lyme disease, in which case a prescription for doxycycline might be appropriate to have on hand. When prescribing antibiotics, discuss allergies and seek antibiotics that can be used for multiple conditions.
Corticosteroids such as prednisone can be prescribed as a short-term course for skin eruptions due to poison ivy or poison oak exposure in sensitive individuals. Hikers with asthma should have a dose of corticosteroids along with them.
For routine medications, hikers should carry enough of a supply with them to last for the entire hike. This includes inhalers for asthma, hypertension medications, oral and injectable hypoglycemics for patients with diabetes, non-sedating antihistamines for environmental allergies, thyroid medications, and other medications that the hiker usually takes. There should be a discussion about nonessential medications or those that can be skipped during the hike. Special attention should be given to drugs such as blood thinners, antidepressants, seizure medications, and migraine medications. Drugs that require regular blood levels to be drawn need to be discussed, and plans made for this intervention while on the trail.
All hikers should be current with their tetanus immunization (Td or Tdap), flu shots, and COVID-19 vaccinations. A series of hepatitis A vaccines (2 doses for lifetime protection) is strongly encouraged due to the risk of acquiring this condition when on the trail.
Final Planning Considerations
Hikers should consider the use of an emergency satellite device. Some devices, such as InReach and Spot, allow the hiker to notify someone on the daily start and end of the hike. Family and friends at home can follow their progress. If there is an emergency, these devices can send an SOS. Some of these devices communicate via satellite, allowing for text communication. If the hikers is using a mapping or trail app, they should make sure they know how to use it before they start.
Encourage the hiker to take as light a pack as possible and to clearly determine what needs to go with them and what they consider luxury items that perhaps can stay behind. The hiker should consider why they want to do this endeavor and what are their goals for this, and what will happen if they don't complete their entire proposed journey.
"
["post_title"]=>
string(36) "Your Patient is Going on a Thru-Hike"
["post_excerpt"]=>
string(125) "The lack of understanding of the hardships hikers encounter during and after a thru-hike creates a gap for providers to fill."
["post_status"]=>
string(7) "publish"
["comment_status"]=>
string(6) "closed"
["ping_status"]=>
string(6) "closed"
["post_password"]=>
string(0) ""
["post_name"]=>
string(36) "your-patient-is-going-on-a-thru-hike"
["to_ping"]=>
string(0) ""
["pinged"]=>
string(0) ""
["post_modified"]=>
string(19) "2024-04-12 10:33:13"
["post_modified_gmt"]=>
string(19) "2024-04-12 14:33:13"
["post_content_filtered"]=>
string(0) ""
["post_parent"]=>
int(0)
["guid"]=>
string(41) "https://www.clinicaladvisor.com/?p=182899"
["menu_order"]=>
int(0)
["post_type"]=>
string(4) "post"
["post_mime_type"]=>
string(0) ""
["comment_count"]=>
string(1) "0"
["filter"]=>
string(3) "raw"
}
[2]=>
object(WP_Post)#7087 (24) {
["ID"]=>
int(182882)
["post_author"]=>
string(5) "45524"
["post_date"]=>
string(19) "2024-04-12 09:54:27"
["post_date_gmt"]=>
string(19) "2024-04-12 13:54:27"
["post_content"]=>
string(13940) "
A recent national health survey showed that the estimated prevalence of irritable bowel syndrome (IBS) ranges between 4.7% and 5.3%, with the prevalence being higher than that of previous estimates.1
Considered a disorder of the gut-brain interaction (previously referred to as a functional gastrointestinal disorder) characterized by abdominal pain and abnormal bowel habits, IBS has further been classified based on predominant stool form in more than 25% of bowel movements. The categories include: IBS with constipation (IBS-C), IBS with diarrhea (IBS-D), and IBS with mixed bowel habits. With this, IBS often requires multidisciplinary management.1,2
Why Use Antidepressants for IBS?
The 2021 American College of Gastroenterology (ACG) guideline update for IBS management3 states that tricyclic antidepressants (TCAs) — also referred to as neuromodulators — may be used to manage global IBS symptoms. Clinicians can recommend gut-directed psychotherapies to patients with IBS after weighing their safety and efficacy, as well as the type of IBS. Research has shown that patients with IBS-D may have a better response to TCAs because of their anticholinergic properties that are known to improve diarrhea; however, all patients with IBS being considered for TCA therapy must be started on a low dose with a gradual dose titration upward. The role of selective serotonin reuptake inhibitors (SSRIs) in IBS has also been discussed in some studies.3,4
A 2023 study (ATLANTIS; ISRCTN48075063) published in The Lancet specifically discussed the use of low-dose amitriptyline (10-30 mg) as a second-line treatment for IBS.5
"
Patients need to know that medications can have multiple purposes — neuromodulators can treat anxiety but also reduce the pain of IBS.
“Amitriptyline was significantly more effective than placebo for people with IBS in primary care who had experienced no benefit from first-line treatments (changes in diet, fiber, laxatives, antidiarrheal agents, or antispasmodic agents),” noted Professor Alexander Ford, the lead author of the ATLANTIS study, professor of gastroenterology, and honorary consultant gastroenterologist at Leeds Institute of Medical Research at St James, University of Leeds and Leeds Gastroenterology Institute, and Leeds Teaching Hospitals Trust, UK. “The effect was seen across all subtypes of IBS and was not accompanied by a change in mood scores, meaning that amitriptyline is not acting as an antidepressant in IBS but is having its effects on gut motility and pain sensation.”
Dr Ford concluded that, “[General practitioners] should offer amitriptyline to patients with IBS who have not experienced a benefit with first-line treatments.”
Considerations for Providers While Treating IBS With Antidepressants
We received expert insights on the use of antidepressants for IBS treatment and what providers should know before prescribing these medications for patients in gastroenterology.
The gastroenterology perspective below was provided by Douglas A. Drossman, MD, professor emeritus of medicine and psychiatry at the Division of Gastroenterology and Hepatology at University of North Carolina (UNC); founder and co-director at UNC Center for Functional GI and Motility Disorders; and founder, president emeritus, and CEO of the Rome Foundation.
Douglas A. Drossman, MD
One of the first things that comes up for me from a gastrointestinal perspective is the stigma attached to patients being prescribed antidepressants, which is why [the Rome Foundation] reframed these medications and called them “neuromodulators”6 that act on the brain-gut axis and not necessarily on the psychiatric profile. It’s important for providers to explain these medications as “altered physiology”; there is a dysregulation of the brain-gut control mechanism leading to symptoms of pain, nausea, and vomiting, and these neuromodulators reverse that.
There are different classes of these neuromodulators or antidepressants for gastroenterology. For example, SSRIs can enhance motility and alleviate constipation, a side effect being diarrhea, but a TCA would also treat the pain and slow down the bowel and treat diarrhea.4
We did a survey of 600 gastroenterologists and most of them were familiar with TCAs, but were much less familiar with SSRIs or SNRIs. Most of their [dilemma] about treatment was they didn’t know what and how to use these medications, and that’s very important to address.
When patients with IBS receive a single medication and are not getting better, you can combine medications. This is where psychiatrist consults can be of help, for modifying the dosage or adding a second medication called augmentation.
The psychiatry perspective below was provided by W. Scott Griffies, MD, associate consulting professor, Duke Psychiatry and Behavioral Sciences.
W. Scott Griffies, MD
A significant percentage of the patients in the ATLANTIS trial5 had anxiety and depression, in addition to IBS, which do not respond to low-dose amitriptyline. So, the comorbidities are something that need to be thought about, and additional treatment may be needed in some cases and referrals to psychiatrists and psychologists would be very helpful and appropriate.
Along those lines, a lot of these are central sensitizing disorders so they overlap with a number of other central sensitizing disorders, such as fibromyalgia and migraines, which also need to be addressed. Many patients with gut-brain interactions have trauma that would qualify for psychiatric treatment.
Review of Safety and Efficacy of Antidepressants for IBS
A review6 by researchers at the University of Leeds, UK, regarding the management of IBS showed that central neuromodulators, including TCAs and SSRIs, resulted in a higher incidence of total adverse events. However, the use of central neuromodulators can be considered when first-line treatments are inadequate. Authors of the review also noted that TCAs may be preferred to SSRIs at low doses (for example, 10 mg at night due to risk for drowsiness), with dose titration up to 50 mg, depending on patient response. Doses greater than 50 mg may be associated with higher rates of adverse events.6
Discussing the overall safety of antidepressant medications, Dr Drossman noted, “The problem with looking at these medications for IBS is they haven’t been well-studied. The only ones that have been well-studied are the TCAs, of which we may use one-thirds [sic] to one-fifth of the dose used in psychiatry and are actually quite safe. However, there are side effects like dry mouth, blurry vision, and constipation. But overall, the side effects are nothing to be too concerned about. The SSRIs for anxiety may cause diarrhea and night sweats; with duloxetine, the side effect is nausea and rarely constipation. But when doses are low, they are generally quite safe.”7
Assessing safety data from the ATLANTIS trial,5 the majority of participants reported at least 1 mild to severe side effect at 3 and 6 months of amitriptyline use for IBS (97% and 99%, respectively), followed by at least 1 moderate to severe side effect in the same time periods (81% and 77%, respectively). The most common side effects reported at any frequency included drowsiness, dry mouth, and diarrhea.5
If treatment response is suboptimal, augmentation with a second agent may be considered after the dose has been increased. For example, adding an antipsychotic medication, such as quetiapine, to existing IBS treatment may improve anxiety and sleep disturbances.7 Dr Griffies also spoke about the importance of augmentation in psychiatry and why it may be useful in gastroenterology, though it may be more challenging for some patients with IBS than others.
Emphasis on Provider-Patient Communication
Timely, appropriate, and evidence-based management of IBS symptoms is important to improve outcomes and patient satisfaction.6
“The first thing I would do [when considering antidepressant treatment for IBS] is get information from the patient, such as their history of medications. It’s much easier to respond to preconceptions rather than give them a litany of information and not know whether they have prior biases,” Dr Drossman indicated. Of note, a paper by Dr Drossman and colleagues refers to establishing a “therapeutic relationship” when prescribing neuromodulator treatment to patients with gut-brain interaction disorders.7
Communication goals should be aimed at improving patient acceptance and adherence.“ For example, some patients may express that ‘these medications may alter [their] mind,’ to which providers can say that ‘[these medications] are not intended to alter the mind; they are used in psychiatry in higher doses to treat conditions like anxiety and depression,” Dr Drossman said. “But we’re using it in lower doses to normalize pain sensitivity and raise sensation threshold through neurotransmitters working on the gut-brain axis. Patients need to know that medications can have multiple purposes — neuromodulators can treat anxiety but also reduce the pain of IBS.”
“Overall, educating patients should be an iterative process,” he concluded. “In addition, gastroenterologists need to become familiar with these medications because they have been shown to be effective.
Collaboration between gastroenterology and psychiatry providers to provide appropriate treatment for this population may be valuable.
"
["post_title"]=>
string(62) "Antidepressants for IBS: What Gastroenterologists Need to Know"
["post_excerpt"]=>
string(176) "First-line treatments for irritable bowel syndrome are not always effective. We spoke with 3 experts who explain the success of using antidepressants to help patients with IBS."
["post_status"]=>
string(7) "publish"
["comment_status"]=>
string(6) "closed"
["ping_status"]=>
string(6) "closed"
["post_password"]=>
string(0) ""
["post_name"]=>
string(23) "antidepressants-for-ibs"
["to_ping"]=>
string(0) ""
["pinged"]=>
string(0) ""
["post_modified"]=>
string(19) "2024-04-12 09:54:37"
["post_modified_gmt"]=>
string(19) "2024-04-12 13:54:37"
["post_content_filtered"]=>
string(0) ""
["post_parent"]=>
int(0)
["guid"]=>
string(41) "https://www.clinicaladvisor.com/?p=182882"
["menu_order"]=>
int(0)
["post_type"]=>
string(4) "post"
["post_mime_type"]=>
string(0) ""
["comment_count"]=>
string(1) "0"
["filter"]=>
string(3) "raw"
}
[3]=>
object(WP_Post)#7069 (24) {
["ID"]=>
int(182740)
["post_author"]=>
string(5) "45391"
["post_date"]=>
string(19) "2024-04-11 09:00:00"
["post_date_gmt"]=>
string(19) "2024-04-11 13:00:00"
["post_content"]=>
string(473) "
A 62-year-old man requests removal of a skin lesion on his abdomen. The patient reports that the lesion has been present for approximately 2 months and is frequently traumatized by clothing. The patient’s medical history is positive for obesity, hypertension, and diabetes. Physical examination reveals a 0.5 cm hyperkeratotic projection on an erythematous base. Scattered seborrheic keratosis are noted on his trunk.
"
["post_title"]=>
string(45) "DermDx: Hyperkeratotic Projection on Red Base"
["post_excerpt"]=>
string(81) "A 62-year-old man requests removal of a hyperkeratotic projection on his abdomen."
["post_status"]=>
string(7) "publish"
["comment_status"]=>
string(6) "closed"
["ping_status"]=>
string(6) "closed"
["post_password"]=>
string(0) ""
["post_name"]=>
string(41) "dermdx-hyperkeratotic-projection-red-base"
["to_ping"]=>
string(0) ""
["pinged"]=>
string(0) ""
["post_modified"]=>
string(19) "2024-04-10 10:15:18"
["post_modified_gmt"]=>
string(19) "2024-04-10 14:15:18"
["post_content_filtered"]=>
string(0) ""
["post_parent"]=>
int(0)
["guid"]=>
string(69) "https://www.clinicaladvisor.com/?post_type=hm-slideshow&p=182740"
["menu_order"]=>
int(0)
["post_type"]=>
string(12) "hm-slideshow"
["post_mime_type"]=>
string(0) ""
["comment_count"]=>
string(1) "0"
["filter"]=>
string(3) "raw"
}
}