Obstructive sleep apnea (OSA) is a disease process wherein the upper airway repeatedly collapses or becomes obstructed during sleep, which can induce intermittent hypoxemia.1,2 Obstructive sleep apnea leads to complete or partially reduced airflow, resulting in frequent awakenings that a person may or may not be aware of. This cyclic process of sleep disruption causes sleep fragmentation and results in poor sleep quality.
Obesity is a potent risk factor for the development and progression of OSA and is common in the US, affecting nearly 40% of the population.1,5 Despite the high prevalence of obesity and the knowledge that obesity is a significant risk factor for OSA, it is estimated that 80% of adults with OSA remain undiagnosed.5 Screening and evaluating patients with known risk factors for OSA should be an essential part of preventive medicine within the US, as it could reduce the healthcare burden and complications related to untreated OSA.
Clinicians should be aware of the serious complications associated with untreated OSA. Obstructive sleep apnea may significantly increase the risk for coronary artery disease, atrial fibrillation, cerebrovascular accident, congestive heart failure, resistant hypertension, and mortality.6-8 Patients with untreated OSA can also experience excessive daytime sleepiness, higher rates of depression, and an increased chance of motor vehicle accidents.9-10 In addition to cardiovascular disease and cognitive and behavioral conditions, untreated OSA is a risk factor for diabetes mellitus as well as the development of malignant and non-malignant tumors.11,12
Risk Factors and Associated Symptoms
Patients at risk for OSA should be promptly identified. In addition to obesity, a common risk factor for OSA is older age.13 Muscle tone in the upper airways becomes weaker with age, putting older adults at higher risk for a collapsed airway and leading to apneic events during sleep.
An increase in neck circumference also serves as a risk factor for OSA, as well as a predictor for the severity of OSA.14,15 Patients at increased risk for OSA usually have a neck size greater than 17 inches in men and 16 inches in women. Neck circumference can have a higher association with OSA compared to body mass index (BMI).
Anatomical abnormalities, including skeletal and soft tissue irregularities, can also predispose patients to OSA by narrowing the upper airway. Examples include a retro-positioned mandible, short maxillary length, narrow anterior cranial base, enlarged tongue, longer uvula, and enlarged tonsils.16,18
Patients at risk for OSA may complain of waking up gasping for air, snoring, or having apneic events.19 Additionally, patients can report uncontrolled daytime tiredness, morning headaches, difficulty concentrating and memory impairment, irritability, nocturia, decreased libido, and erectile dysfunction.19-21
Screening Tools and Diagnostics
The United States Preventative Service Task Force (USPSTF) currently concludes that there is insufficient evidence for the benefits or harms in routinely screening asymptomatic adult patients for OSA.22 However, this recommendation only applies to patients who are asymptomatic or without risk factors, which is a key distinction. Patients with risk factors or associated symptoms should be screened for OSA. In population surveys previously conducted, 86% to 95% of individuals with clinically significant OSA reported no prior OSA diagnosis, and the majority of primary care clinicians do not screen patients for OSA.22,23 Additionally, it is not unusual for patients to ignore or not talk about symptoms that may be concerning for OSA with their provider.
There are multiple questionnaires including the Epworth Sleepiness Scale (ESS), Berlin questionnaire (BQ), and the STOP-Bang questionnaire (SBQ) to screen for OSA. The SBQ is an 8-item survey that evaluates snoring, tiredness, observed apneas, blood pressure, BMI, age, neck circumference, and gender.24 The SBQ questionnaire is one of the most sensitive assessment tools available, making it a preferred screening method.The SBQ assesses risk factors and symptoms, while the ESS assesses daytime sleepiness by quantifying the likelihood of falling asleep in 8 different situations, such as watching television or sitting quietly as a passenger in a car.24 It is important to note that although questionnaires can be useful in screening for OSA, these are not diagnostic tools and should not replace diagnostic studies.25
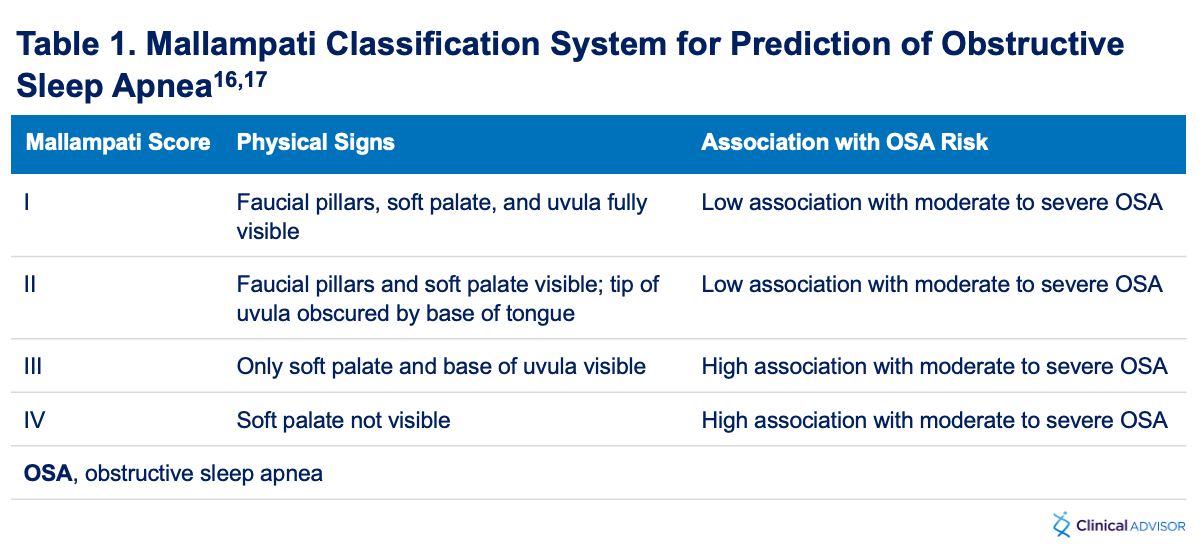
When evaluating patients for a narrow upper airway, using the Mallampati classification system can help determine if patients are at risk for OSA (Table 1). A Mallampati classification of III or IV has a high association with OSA and can be used as a predictive assessment for patients at risk.16 A Mallampati classification of III is when only the base of the uvula is visible, and a Mallampati classification of IV is when the soft palate is not visible. This exam is performed by evaluating the patient’s posterior pharynx when they are sitting in the upright position, mouth open, with their tongue protruding.17
Patients with OSA risk factors, signs and symptoms, or abnormal screening results should undergo diagnostic testing. An in-laboratory polysomnography (PSG) is currently the gold standard diagnostic test; however, not all patients require an in-laboratory PSG.26 Instead, some patients can undergo home sleep apnea testing (HSAT), but there are certain restrictions to this.
The American Academy of Sleep Medicine (AASM) reports home sleep apnea testing should be reserved only for patients at increased risk of moderate to severe OSA, which would include patients who experience excessive daytime fatigue and at least 2 of the following criteria: diagnosed hypertension, habitual snoring, or witnessed apnea or gasping or choking.25 The diagnostic impetus for ordering an HSAT should be to confirm highly suspected OSA.
If the results of the HSAT are technically inadequate, negative, or inconclusive, then AASM recommends performing an in-lab PSG—further supporting that HSAT should only be used in patients highly suspected of having OSA, in order to avoid unnecessary repeat testing. Certain patients who are at an increased risk for complex forms of sleep apnea, including those with a history of stroke, cardiac or respiratory disease, neuromuscular disease, or opioid usage, should undergo in-lab PSG testing.25 Additionally, certain workers (ie, police officers, airline pilots, truck drivers, taxi or ride-sharing drivers, etc) as well as patients suspected to have non-respiratory sleep disorders (ie, limb movement disorders, parasomnias, narcolepsy, etc) should also undergo in-lab PSG testing.
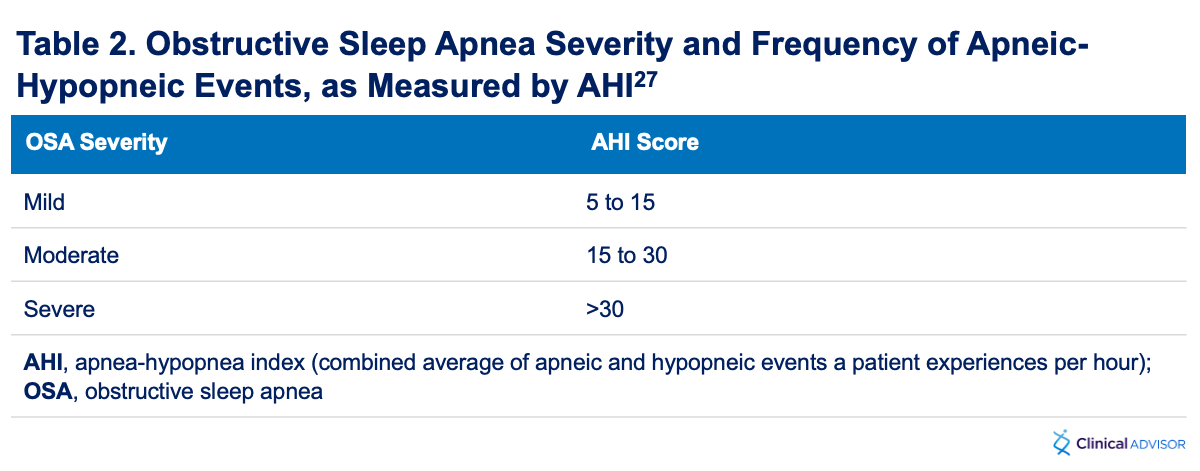
The diagnosis of sleep apnea is based on the patient’s apnea-hypopnea index (AHI), which is a combined average of apneic and hypopneic events a patient experiences per hour.27 An apneic event occurs when there is complete or nearly complete cessation of airflow (90% or greater) for a minimum of 10 seconds; a hypopneic event occurs when airflow decreases by at least 30% and lasts for 10 seconds. Mild OSA consists of an AHI between 5 and 15; moderate OSA consists of an AHI between 15 and 30; and severe OSA is diagnosed with an AHI greater than 30 (Table 2). Apneic events will be reported as either obstructive, central, or mixed. If patients are experiencing multiple central or mixed apneic events this could be indicative of central or mixed sleep apnea. For patients diagnosed with uncomplicated OSA based on AHI, treatment may be initiated without a titration study.28
Treatment
Positive airway pressure (PAP) is the initial treatment of choice for OSA.29 If the patient is in agreeance with PAP therapy and does not have significant comorbidities, such as neuromuscular disease, cardiac disease, lung disease, chronic opiate use, or other medical conditions, then PAP therapy using automatic positive airway pressure (APAP) can be considered. Automatic positive airway pressure devices provide continuous positive airway pressure but can automatically adjust to the patient’s needs by increasing pressure when more airway resistance is detected and decreasing pressure in the presence of less airway resistance.
"
Patients with untreated OSA can also experience excessive daytime sleepiness, higher rates of depression, and an increased chance of motor vehicle accidents.
Alternatively, patients can undergo a titration study to determine which pressures are needed to control their sleep apnea. Once treatment is started, a compliance report from the PAP device will be generated, which provides data that includes usage time and air leakage (if present), as well as AHI, PAP settings, and other data. This information must be evaluated at follow-up appointments to ensure adherence and that the patient’s sleep apnea is controlled. Patients who have ongoing uncontrolled OSA should be referred to a sleep medicine specialist for further evaluation and treatment. If the provider is unfamiliar with the treatment for OSA, patients can be referred to a sleep medicine specialist.
For patients who fail or do not tolerate PAP therapy, second-line treatment options for OSA include mandibular advancement devices, tongue-retaining devices, and surgery for anatomical abnormalities. There is also a newly developing therapy that involves stimulation therapy using a lead that attaches to the hypoglossal nerve, which treats OSA by causing the tongue to protrude.30
Conclusion
Obstructive sleep apnea is an underrecognized and underdiagnosed disease with the potential for serious implications if left untreated, including cardiovascular and pulmonary complications, cognitive impairment and behavioral conditions, metabolic disease, stroke, cancer, and even death. The risk factors associated with OSA are not uncommon and include obesity, which has a critical role in the disease. Primary care providers are at the forefront of recognizing and screening at-risk patients, ordering diagnostic testing, and initiating therapy. Addressing OSA is more than just treating a disease: it is an essential part of preventative medicine, as it has the potential to prevent or reduce the burden of many other serious medical conditions.
Colorectal cancer (CRC), a collective term for colon and rectal cancers, is the third leading cause of cancer-related deaths among men and the fourth leading cause among women in the United States.1
However, there are ways to reduce risk for CRC — and even stop it from spreading. Screening methods are designed to detect and, in some cases, remove precancerous or cancerous growths in the body.
The American Cancer Society (ACS) and the US Preventive Services Task Force recommend that adults at average risk for CRC begin screening at 45 years of age and continue through 75 years of age.2,3
Individuals are considered at “average risk” if they do not have any of the following2:
Personal history of CRC or certain kinds of polyps;
Family history of CRC;
Confirmed or suspected CRC syndrome, such as Lynch syndrome (hereditary nonpolyposis colon cancer);
Inflammatory bowel disease (Crohn disease or ulcerative colitis); or,
Personal history of receiving radiation to the abdomen or pelvic area for previous cancer treatment.
An individual who does have any of the items listed above may be at increased risk for CRC and may need to start screening before 45 years of age.2
From 76 to 85 years of age, individuals should speak with their doctor and consider factors such as overall health, life expectancy, and screening history.2,3 Beyond 85 years of age, the ACS does not recommend further screening.2
Testing for Colon Cancer With Visual Exams
There are 3 types of visual exams that look at the rectum and large intestine (colon) to screen for cancer.2 Colonoscopy is the gold standard for CRC screening, but, if necessary, your doctor may recommend other methods.
Colonoscopy
During a colonoscopy, a doctor inserts a tube, called a colonoscope, through the rectum and into the colon to search for abnormal growths, such as polyps, along the lining of the intestines. The doctor may also remove polyps during the procedure to prevent them from turning into cancer. The polyps may later be examined in a biopsy to confirm if cancer is present.4,5 A colonoscopy may be performed as a follow-up test to other screening methods.
Frequency: Every 10 years2
CT Colonography (Virtual Colonoscopy)
Computed tomography (CT) colonography, also referred to as “virtual colonoscopy,” uses a series of X-rays to produce computer-generated images of the colon. A doctor will examine the images for signs of precancerous or cancerous polyps. Before the procedure, you will be asked to drink a liquid with a dye that serves as contrast medium to help make the colon visible during radiation.7 In some cases, IV contrast is used instead.6 During the procedure, a doctor will insert a tube into the rectum to inflate the colon with carbon dioxide for better imaging. Then, the doctor performs CT scans to visualize the colon.5-7 A follow-up colonoscopy is necessary if the colonography finds abnormal results.9
Frequency: Every 5 years2
Flexible Sigmoidoscopy
A doctor inserts a tube, called a sigmoidoscope, into the rectum and lower portion of the colon to look for abnormal growths of tissue, such as polyps.5 During the procedure, the doctor may also remove polyps or tissue to later examine for cancer. If precancerous polyps or cancer are detected, you will be asked to schedule a colonoscopy, since a sigmoidoscopy only examines a portion of the colon.8,9
Frequency: Every 5 years2
Testing for Colon Cancer With Stool Tests
Unlike colonoscopy, which can help prevent CRC via precancerous polyp removal, stool tests detect CRC after it has developed. There are 3 types of stool tests, of which 2 detect blood in the stool and the third detects blood in addition to DNA biomarkers for cancer in the stool.9 Stool tests are performed at home but may need to be done more frequently than visual exams.8 For all stool tests, abnormal results require a follow-up colonoscopy visit.9
Guaiac-Based Fecal Occult Blood Test (gFOBT)
The gFOBT uses the chemical guaiac to detect blood in the stool. Before the test, your doctor may ask you to avoid consuming certain foods and drugs, which may affect test results.8,9 You will receive an at-home test kit, which contains tools and instructions on how to collect a small stool sample. Then, you mail the sample back to the doctor or laboratory, where guaiac is used to detect blood in the stool.5,10
Frequency: Every year2
Fecal Immunochemical Test (FIT)
The FIT uses antibodies to detect blood in the stool. You will receive an at-home test kit, which contains a collection tube or cards. You will collect a small stool sample and return it to a doctor’s office or laboratory via mail or in person. At the laboratory, a liquid is added to the stool sample and then processed in a machine containing antibodies, which detect blood in the stool.10
Frequency: Once a year2
FIT-DNA Test
The FIT-DNA test, or “stool DNA test,” uses both the FIT and a test that detects DNA biomarkers, or changes, in the stool from cancer or polyp cells.5,9 Using an at-home test kit, you will collect an entire stool sample and mail it back to a laboratory, where it will be analyzed for DNA alterations and blood in the stool.9,11
Frequency: Every 3 years2
Frequently Asked Patient Questions
Will I experience discomfort during colonoscopy?
Colonoscopy is performed using sedation, so you will likely sleep through the procedure.16 Most patients report discomfort with the process leading up to colonoscopy: bowel preparation. You will be instructed to take laxatives and follow a liquid diet, which will help empty the colon of all waste.4
Why is bowel preparation important for colonoscopy?
Thoroughly cleansing stool from the colon helps the doctor clearly detect precancerous and cancerous tissue, which also decreases the need for repeat colonoscopies. A doctor may choose not to proceed with the procedure due to inadequate bowel preparation, which increases the risk for false-negative results and perforation.4
Besides screening methods, what else can I do to help prevent CRC?
Healthy lifestyle choices can help lower your risk for CRC. Consult with your doctor about the information below:
Diet
Research shows that red meat, such as beef, lamb, or pork, and processed meats, such as sausage, hotdogs, or deli meat, are associated with an increased risk for CRC.12 In contrast, a diet high in fiber, such as fruits, vegetables, and whole grains, is associated with a reduced risk for CRC.13
Exercise
Regular physical activity can be beneficial. Studies show that exercise can help decrease your risk for CRC.14
Weight management
Overweight and obesity are linked to an increased risk for CRC among both men and women.15
A 16-year-old adolescent presents for treatment of a facial breakout. The condition has been increasing in severity over the past year. Her family history is positive for moderate to severe acne and her father was treated with a course of isotretinoin while a college student. She has never taken birth control pills and is on no oral medications. Several weeks ago, she self-medicated with an over-the-counter benzoyl peroxide gel but found the preparation too irritating. Examination reveals multiple 1- to 2-mm whitish papules.
"
["post_title"]=>
string(35) "DermDx: Whitish Papules on Forehead"
["post_excerpt"]=>
string(135) "A 16-year-old adolescent presents for treatment of a facial breakout. The condition has been increasing in severity over the past year."
["post_status"]=>
string(7) "publish"
["comment_status"]=>
string(6) "closed"
["ping_status"]=>
string(6) "closed"
["post_password"]=>
string(0) ""
["post_name"]=>
string(31) "dermdx-whitish-papules-forehead"
["to_ping"]=>
string(0) ""
["pinged"]=>
string(0) ""
["post_modified"]=>
string(19) "2024-04-25 15:14:04"
["post_modified_gmt"]=>
string(19) "2024-04-25 19:14:04"
["post_content_filtered"]=>
string(0) ""
["post_parent"]=>
int(0)
["guid"]=>
string(69) "https://www.clinicaladvisor.com/?post_type=hm-slideshow&p=183605"
["menu_order"]=>
int(0)
["post_type"]=>
string(12) "hm-slideshow"
["post_mime_type"]=>
string(0) ""
["comment_count"]=>
string(1) "0"
["filter"]=>
string(3) "raw"
}
[3]=>
object(WP_Post)#7064 (24) {
["ID"]=>
int(183491)
["post_author"]=>
string(5) "45391"
["post_date"]=>
string(19) "2024-04-24 14:50:41"
["post_date_gmt"]=>
string(19) "2024-04-24 18:50:41"
["post_content"]=>
string(9434) "
From beneath a warm swaddling of blankets, Marisa Fine had no way of knowing that her newborn son had a foot deformity. But about 2 weeks after he was born, something looked odd during bath time.
When her son was 1 month old, Marisa and her husband decided to see a clinician to get answers as to why their son’s feet appeared deformed. At their local hospital in Israel, they received a diagnosis for their son: metatarsus adductus (MTA).
Treatment Options for MTA
MTA is a congenital condition that occurs in between 1 and 3 in 1000 births. In infants without MTA, a line that bisects the heel will also bisect the space between the second and third toe. In infants with mild MTA, the line will bisect the third toe; in moderate cases, the line will bisect the space between the third and fourth toe, and in severe cases, the line will bisect the space between the fourth and fifth toe.1
Credit: Courtesy of UNFO Med. Ltd
"
Dr Daizade is hopeful that patients around the world will benefit from access to orthotic devices to treat MTA.
Historically, parents have had 3 treatment options to correct their child’s MTA. Since the condition in many cases self-corrects, parents are often given the option to wait and see if treatment is necessary. If MTA does not self-correct or if parents elect to initiate treatment immediately, then the child can undergo a casting process to straighten their feet or opt for wearing modified shoes or braces.
“I didn’t want to take a gamble on my child's feet or legs,” she said. “If it doesn't correct itself, there could be a problem later on…I wanted to be able to do something. I didn't want to just wait and I didn't want to do casting. I looked into it and it's so painful for the child, it's uncomfortable, and it's not aesthetic… it's just very problematic.”
Not only are novel orthotic devices effective in treating MTA in children aged 10 months or younger,2 they are also more convenient for parents since they are easy to use and resemble an infant shoe, reducing social burden associated with MTA treatment.1
“The remarkable ease and simplicity in treating infants with UNFO orthotic splints introduces a new reality, allowing for the treatment of any type of MTA without age limitations and the risk of lifelong deformities,” said Izak Daizade, MD, a leading expert in orthopedic surgery with more than 30 years of experience dedicated to treating newborns, including Marisa’s son. “The considerable therapeutic success observed in extensive studies further validates this innovative approach. Comparatively, the method of treatment involving a series of casts pales in effectiveness when compared to the treatment with UNFO casts.”
Serial casting is typically completed over a 6 to 8-week span with casts changed every 2 weeks; Dr Daizade explained that this process is burdensome for infants with MTA and their parents.
“Muscles may temporarily weaken, and there may be joint stiffness after ankle and knee fixation,” Dr Daizade said. “Care must be taken to keep the cast dry during bathing, and pressure sores may develop beneath it. Swelling in the foot because of impaired blood flow and hygienic discomfort, especially with long leg casts, are common.”
Unlike casts, orthotic devices used to treat MTA operate below the ankle to allow the joint to move freely, preventing stiffness. Skin complications are less likely to occur in patients who use orthotics vs casts, as parents have the opportunity to monitor the infant’s skin daily during sock changes and bath time.
How to Use Novel Orthotic Devices for MTA
While protocol varies depending on the severity of the infant’s MTA, orthotic devices are meant to be used continuously for 6 to 8 weeks, followed by 6 to 8 weeks of nighttime use on average.3
On the first day of bracing, the device should be removed every 2 hours for 10 minutes; the brace should not be removed on the first night unless the brace causes irritation to the infant.3
The second day should follow the same pattern as the first with removal every 2 hours for 10 minutes; however, the brace can be removed after the infant’s evening bath on the second day. Over the next 12 days, the infant should wear the brace 24 hours a day except for 2 removals: once in the morning, during which the infant’s socks should be changed, and once in the evening for bath time.3
At 2 weeks, a clinician will determine optimal next steps. Typically, a second check-up occurs after 6 weeks of continuous use. At this point, the clinician will determine whether the infant still requires 24-hour therapy, or if the patient can switch to 15-hour overnight therapy. A third check-up should take place after 3 weeks of 15-hour overnight therapy; at this time, the clinician will determine if the patient can switch to 12-hour overnight therapy. After 3 weeks of 12-hour overnight therapy, a fourth check-up should take place to determine if the brace is no longer needed.3
If a parent or clinician observes regression at any point in the process, resumption of 24-hour therapy should be considered.3
Expanding Access to Novel Orthotic Devices
Dr Daizade is hopeful that patients around the world will benefit from access to orthotic devices to treat MTA. So far in the United States, patients in Miami and Baltimore have been successfully treated with the device.
With increased awareness of the condition and noninvasive treatment options available, Marisa hopes that more infants will have positive outcomes like her son.
“These children, they don't need to suffer,” Marisa said. “They don't need to have these uncomfortable casts that can be so traumatizing when they're little and there's a better option out there and it doesn't hurt. It's not invasive and it's easy to use. Why would you have your child go through that if they don't have to?”
You’ve read {{metering-count}} of {{metering-total}} articles this month.
We want you to take advantage of everything Clinical Advisor has to offer. To view unlimited content, log in or register for free.
{{login-button}} {{register-button}}
Want to view more content from Clinical Advisor?
Register now at no charge to access unlimited clinical news with personalized daily picks for you, full-length features, case studies, conference coverage, and more.
{{login-button}} {{register-button}}
Want to read more?
Please login or register first to view this content.